Florida Rts 6 Form in PDF
Florida Rts 6 Form in PDF
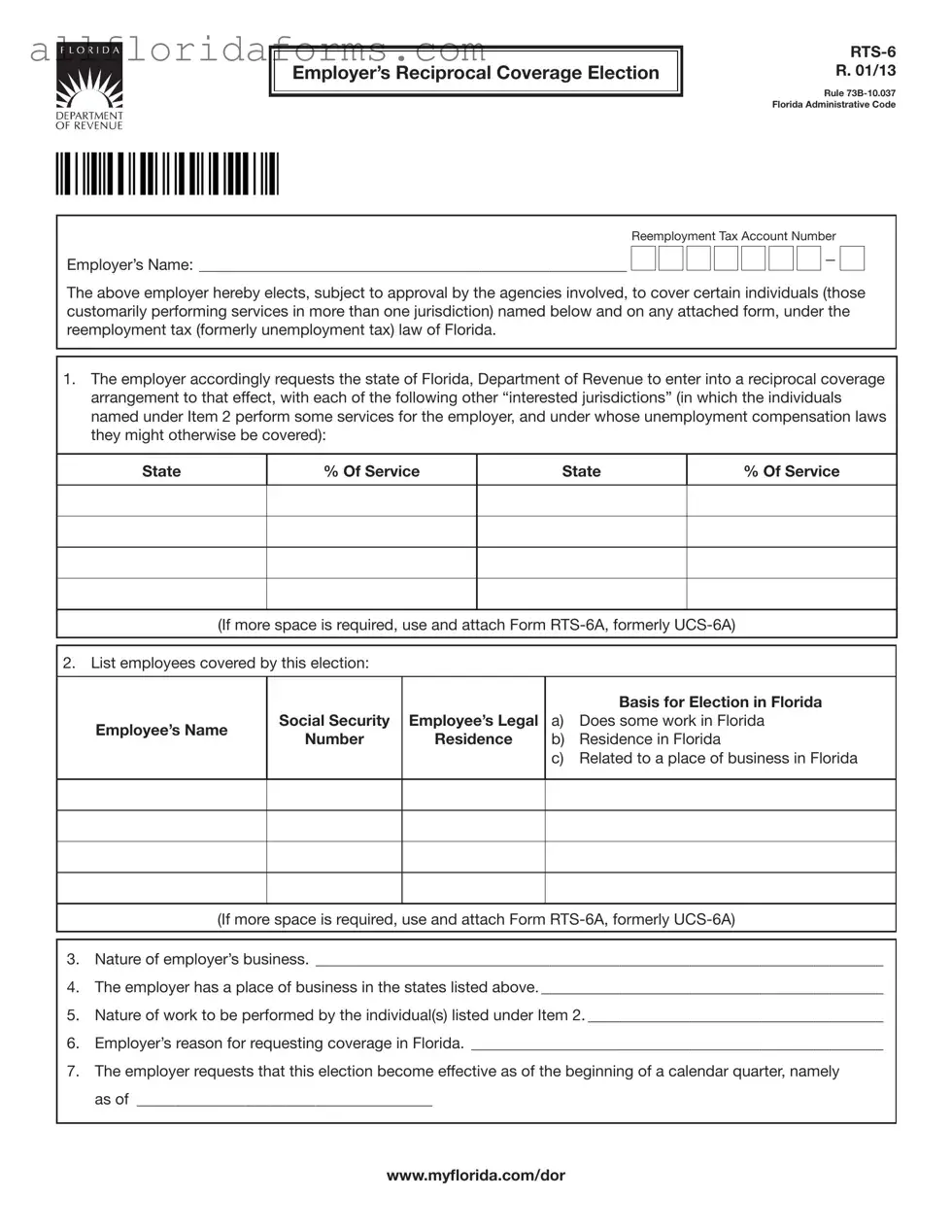
The Florida RTS-6 form, known as the Employer’s Reciprocal Coverage Election, plays a crucial role for businesses operating across multiple states. This form allows employers to elect coverage under Florida's reemployment tax law for certain employees who regularly perform work in more than one jurisdiction. By submitting the RTS-6, employers can request a reciprocal coverage arrangement with other states where these employees provide services. This helps ensure that employees are covered under the appropriate unemployment compensation laws, avoiding potential gaps in their benefits. The form requires employers to list the jurisdictions involved, the employees covered, and the nature of their business. Additionally, it outlines the employer's reasons for seeking coverage in Florida, which could include factors such as the employee's residence or work location. Once approved, this election remains in effect until terminated according to Florida Department of Revenue regulations. Employers must also notify covered individuals of this election and comply with all applicable requirements. The RTS-6 is essential for businesses looking to navigate the complexities of multi-state employment and ensure their employees receive the benefits they deserve.
Employer’s Reciprocal Coverage Election
R. 01/13
Rule
|
Reemployment Tax Account Number |
|||||||||||||
Employer’s Name: _______________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The above employer hereby elects, subject to approval by the agencies involved, to cover certain individuals (those customarily performing services in more than one jurisdiction) named below and on any attached form, under the reemployment tax (formerly unemployment tax) law of Florida.
1.The employer accordingly requests the state of Florida, Department of Revenue to enter into a reciprocal coverage arrangement to that effect, with each of the following other “interested jurisdictions” (in which the individuals named under Item 2 perform some services for the employer, and under whose unemployment compensation laws they might otherwise be covered):
State
% Of Service
State
% Of Service
(If more space is required, use and attach Form
2. List employees covered by this election:
Employee’s Name
Social Security |
Employee’s Legal |
Number |
Residence |
|
|
Basis for Election in Florida
a)Does some work in Florida
b)Residence in Florida
c)Related to a place of business in Florida
(If more space is required, use and attach Form
3.Nature of employer’s business. _________________________________________________________________________
4.The employer has a place of business in the states listed above. ____________________________________________
5.Nature of work to be performed by the individual(s) listed under Item 2. ______________________________________
6.Employer’s reason for requesting coverage in Florida. _____________________________________________________
7.The employer requests that this election become effective as of the beginning of a calendar quarter, namely as of ______________________________________
www.mylorida.com/dor
R. 01/13
Page 2
ELECTION (continued)
8.This election, if approved, shall remain operative, as to the individuals listed herewith, until terminated in accordance with the currently applicable regulations of the Florida Department of Revenue.
9.The employer hereby agrees to give each individual covered by this election a notice thereof, promptly after its approval, on a form to be supplied by the Florida Department of Revenue, and to ile copies thereof with said agency.
10.The employer hereby agrees to comply with any requirements applicable to this election under the Florida Department of Revenue.
11.To prevent this election from denying reemployment assistance/unemployment compensation coverage to workers not listed hereon, the employer hereby agrees with each interested jurisdiction approving this election that it may count the workers covered by this election, and their wages, as if this election did not apply, for the purpose
of determining whether the employer is covered by the law of such jurisdiction and whether any other workers employed by him are covered by said law.
SIGNED, for the employer by: ______________________________________________________________________________
Date: ____________________________________________ Title: _________________________________________________
APPROVAL by the state of Florida, Department of Revenue
The foregoing election is hereby approved, in accordance with the applicable regulations, as submitted by the elect- ing employer.
APPROVED for the state of Florida, Department of Revenue.
By: __________________________________________________
Date: ____________________________________________ Title: _________________________________________________
APPROVED by the interested jurisdiction of _________________________________________________________________
The foregoing is similarly approved.
Name of Agency: ______________________________________
By: __________________________________________________
Date: ____________________________________________ Title: _________________________________________________
NOTE: The employer should submit two (2) signed copies for each jurisdiction listed under item 1, plus two (2) additional copies. All copies should be sent to the state of Florida, Department of Revenue, P.O. Box 6510, Tallahassee, FL
Social security numbers (SSNs) are used by the Florida Department of Revenue as unique identiiers for the administration of Florida’s taxes. SSNs obtained for tax administration purposes are conidential under sections 213.053
and 119.071, Florida Statutes, and not subject to disclosure as public records. Collection of your SSN is authorized under state and federal law. Visit our Internet site at www.mylorida.com/dor and select “Privacy Notice” for more
information regarding the state and federal law governing the collection, use, or release of SSNs, including authorized exceptions.
www.mylorida.com/dor
| Fact Name | Description |
|---|---|
| Form Title | Employer’s Reciprocal Coverage Election RTS-6 |
| Governing Law | Rule 73B-10.037, Florida Administrative Code |
| Purpose | This form allows employers to elect coverage for employees performing services in multiple jurisdictions under Florida's reemployment tax law. |
| Effective Date | The election becomes effective at the beginning of a calendar quarter as specified by the employer. |
| Approval Process | The election must be approved by the Florida Department of Revenue and any interested jurisdictions. |
| Employee Notification | Employers must notify each individual covered by this election promptly after approval. |
| Duration of Election | The election remains effective until terminated per Florida Department of Revenue regulations. |
| SSN Confidentiality | Social Security Numbers are confidential and protected under Florida Statutes, used solely for tax administration. |
Are Net Listings Legal in Florida - It addresses the broker's authority to market the property publicly, ensuring maximum exposure to potential buyers.
Form 6 Florida - Prompt submission after completion is emphasized to facilitate the smooth transition within the SEVIS system and between institutions.