Florida Medical Exemption Vaccine Form in PDF
Florida Medical Exemption Vaccine Form in PDF
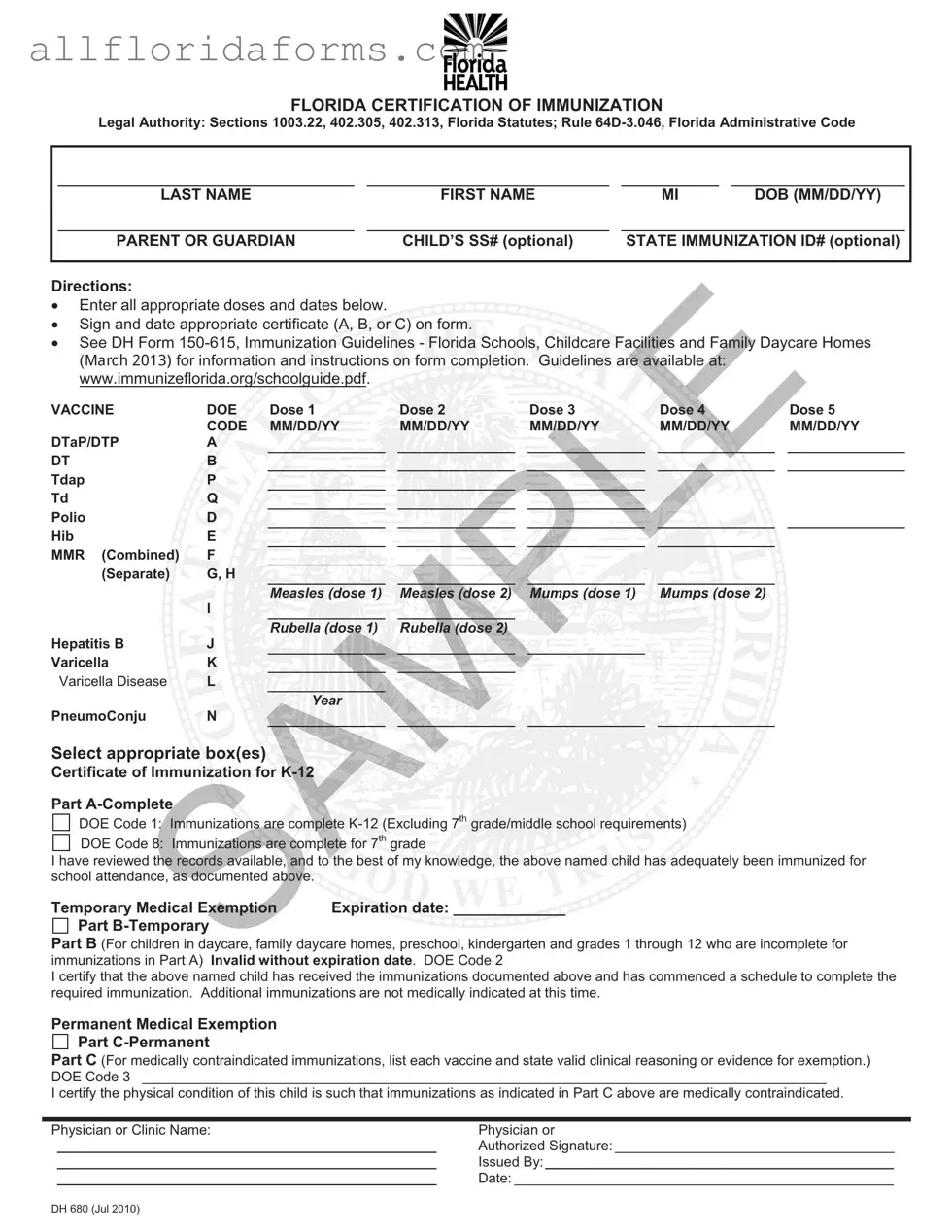
The Florida Medical Exemption Vaccine form serves as a critical document in the state’s immunization process for children attending school and daycare facilities. It is structured to accommodate various scenarios regarding vaccination status, including complete immunization records, temporary exemptions, and permanent medical exemptions. Parents or guardians must provide essential information such as the child’s name, date of birth, and optional social security number. The form outlines specific vaccines, allowing for the documentation of multiple doses and corresponding dates. Additionally, it includes sections for certifying that a child has received all necessary vaccinations or for indicating that a medical exemption applies due to contraindications. This exemption must be supported by valid clinical reasoning, ensuring that the health needs of the child are prioritized. The legal authority for this form is grounded in several Florida statutes and administrative rules, reinforcing its importance within the state's public health framework. For guidance on completing the form, parents can refer to the Department of Health's immunization guidelines, which provide detailed instructions on the immunization requirements for K-12 students and those in daycare settings.

FLORIDA CERTIFICATION OF IMMUNIZATION
Legal Authority: Sections 1003.22, 402.305, 402.313, Florida Statutes; Rule
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
FIRST NAME |
|
MI |
|
DOB (MM/DD/YY) |
|
|
|
|
|
|
|
|
|
|
|
PARENT OR GUARDIAN |
|
CHILD’S SS# (optional) |
|
STATE IMMUNIZATION ID# (optional) |
|
||
|
|
|
|
|
|
|
|
|
Directions:
Enter all appropriate doses and dates below.
Sign and date appropriate certificate (A, B, or C) on form. |
|
|
|
|
|
|
|||||
See DH Form |
|||||||||||
(0DUFK |
for information and instructions on form completion. Guidelines are available at: |
|
|
||||||||
www.immunizeflorida.org/schoolguide.pdf. |
|
|
|
|
|
|
|
|
|||
VACCINE |
|
DOE |
Dose 1 |
|
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
|
CODE |
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
DTaP/DTP |
|
A |
|
|
|
|
|
|
|
|
|
DT |
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tdap |
|
P |
|
|
|
|
|
|
|
|
|
Td |
|
Q |
|
|
|
|
|
|
|
|
|
Polio |
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hib |
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MMR (Combined) |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
(Separate) |
G, H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles (dose 1) |
|
Measles (dose 2) |
|
Mumps (dose 1) |
|
Mumps (dose 2) |
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rubella (dose 1) |
|
Rubella (dose 2) |
|
|
|
|
|
|
Hepatitis B |
|
J |
|
|
|
|
|
|
|
|
|
Varicella |
|
K |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Varicella Disease |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Year
PneumoConju N
Select appropriate box(es)
box(es)
Certificate of Immunization  K-12
K-12
Part
DOE Code 1: Immunizations are complete
DOE Code 8: Immunizations are complete for 7th grade
are complete for 7th grade
I have reviewed the records available, and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.
and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.


Temporary Medical Exemption |
Expiration date: |
Part |
|
Part B (For children in daycare, family daycare homes, preschool, kindergarten and grades 1 through 12 who are incomplete for immunizations in Part A) Invalid without expiration date. DOE Code 2
I certify that the above named child has received the immunizations documented above and has commenced a schedule to complete the required immunization. Additional immunizations are not medically indicated at this time.
Permanent Medical Exemption
Part
Part C (For medically contraindicated immunizations, list each vaccine and state valid clinical reasoning or evidence for exemption.) DOE Code 3 ________________________________________________________________________________________
I certify the physical condition of this child is such that immunizations as indicated in Part C above are medically contraindicated.
Physician or Clinic Name: |
Physician or |
_________________________________________________ |
Authorized Signature: ____________________________________ |
_________________________________________________ |
Issued By:_____________________________________________ |
_________________________________________________ |
Date: _________________________________________________ |
DH 680 (Jul 2010)
| Fact Name | Details |
|---|---|
| Legal Authority | The Florida Medical Exemption Vaccine form is governed by Sections 1003.22, 402.305, and 402.313 of the Florida Statutes, as well as Rule 64D-3.046 of the Florida Administrative Code. |
| Purpose | This form is used to document a child's immunization status for school attendance and to apply for medical exemptions. |
| Expiration Date Requirement | For a temporary medical exemption, an expiration date must be included; otherwise, the exemption is considered invalid. |
| Immunization Codes | The form includes specific codes for various vaccines, such as DTaP, Polio, MMR, and Varicella, which must be documented. |
| Sections of the Form | The form is divided into three parts: Part A for complete immunizations, Part B for temporary exemptions, and Part C for permanent medical exemptions. |
| Physician Certification | A physician or clinic must sign the form, certifying the medical condition that contraindicates immunizations for permanent exemptions. |
| Additional Resources | Guidelines for completing the form can be found on the Florida Department of Health's website, specifically at www.immunizeflorida.org/schoolguide.pdf. |
How Long Does It Take to Become a Cna in Florida - Specifies that failure to notify the Board of changes may delay or result in denial of the application.
Joint Custody in Florida Form - Depending on the respondent's action, the petitioning process branches into default, uncontested, or contested paths.
Form 6 Florida - Authorization from the student for their current international advisor to release necessary information to FIU is requisite for processing.