Florida Kidcare Form in PDF
Florida Kidcare Form in PDF
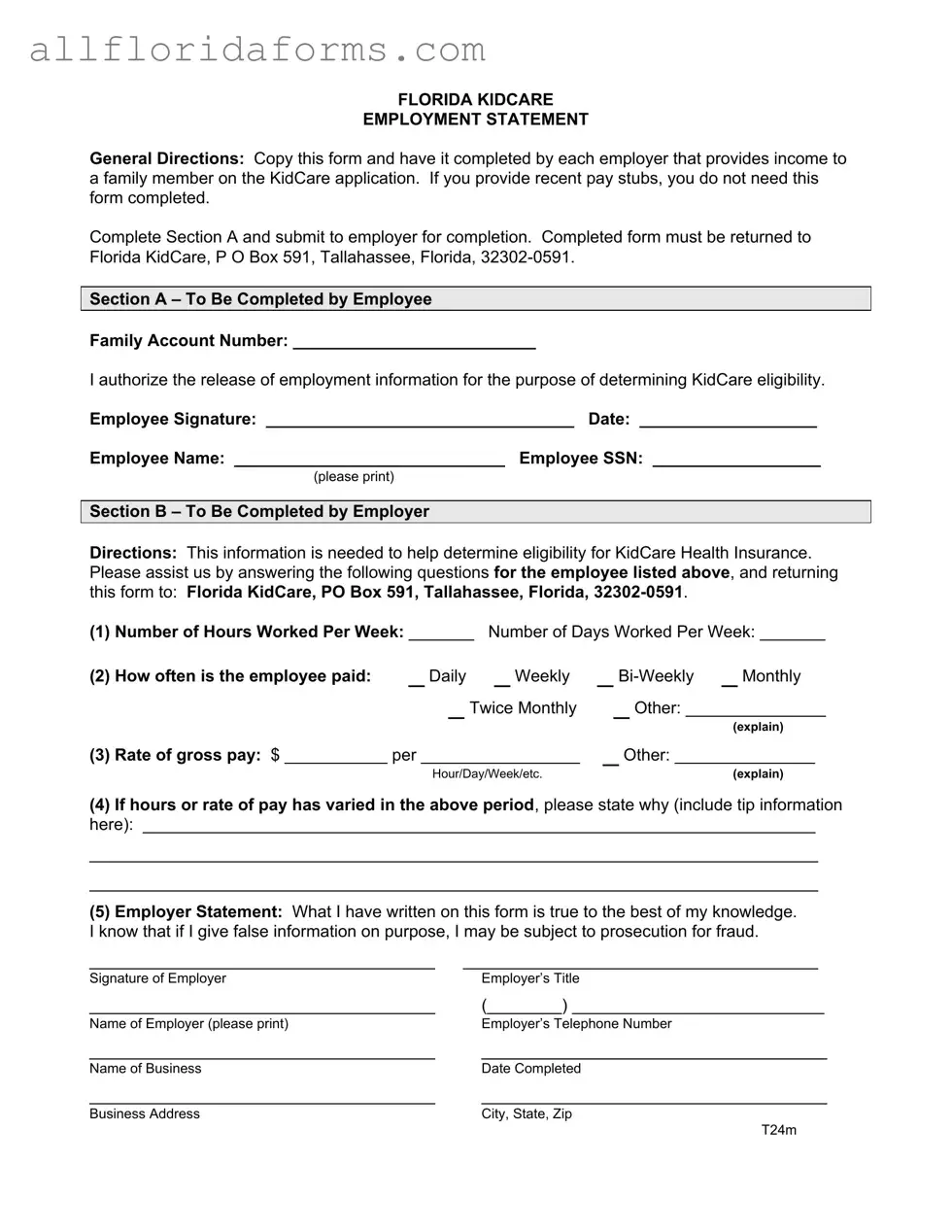
When applying for Florida KidCare, families often encounter the Florida KidCare Employment Statement form, a crucial document in the eligibility assessment process. This form must be completed by each employer providing income to a family member on the KidCare application. For those who can provide recent pay stubs, the form is not necessary. However, if you need to use it, start by filling out Section A, which requires basic employee information and an authorization for the release of employment details. Once completed, this section is submitted to the employer for their input. Section B is then filled out by the employer, who provides essential information such as the number of hours worked per week, payment frequency, and gross pay rate. It’s vital for employers to ensure the accuracy of their responses, as any false information can lead to serious consequences. After the employer completes the form, it should be returned to Florida KidCare at the designated address. Understanding the importance of this form can help streamline the application process and ensure that families receive the health coverage they need.
FLORIDA KIDCARE
EMPLOYMENT STATEMENT
General Directions: Copy this form and have it completed by each employer that provides income to a family member on the KidCare application. If you provide recent pay stubs, you do not need this form completed.
Complete Section A and submit to employer for completion. Completed form must be returned to Florida KidCare, P O Box 591, Tallahassee, Florida,
Section A – To Be Completed by Employee
Family Account Number: __________________________
I authorize the release of employment information for the purpose of determining KidCare eligibility.
Employee Signature: _________________________________ Date: ___________________
Employee Name: _____________________________ Employee SSN: __________________
(please print)
Section B – To Be Completed by Employer
Directions: This information is needed to help determine eligibility for KidCare Health Insurance. Please assist us by answering the following questions for the employee listed above, and returning this form to: Florida KidCare, PO Box 591, Tallahassee, Florida,
(1) Number of Hours Worked Per Week: _______ |
Number of Days Worked Per Week: _______ |
|
(2) How often is the employee paid: |
_ Daily |
_ Weekly _ |
_ Twice Monthly |
_ Other: _______________ |
|
(explain) |
(3) Rate of gross pay: $ ___________ per _________________ |
_ Other: _______________ |
Hour/Day/Week/etc. |
(explain) |
(4)If hours or rate of pay has varied in the above period, please state why (include tip information here): ________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
(5)Employer Statement: What I have written on this form is true to the best of my knowledge. I know that if I give false information on purpose, I may be subject to prosecution for fraud.
_____________________________________ |
______________________________________ |
Signature of Employer |
Employer’s Title |
_____________________________________ |
(________) ___________________________ |
Name of Employer (please print) |
Employer’s Telephone Number |
_____________________________________ |
_____________________________________ |
Name of Business |
Date Completed |
_____________________________________ |
_____________________________________ |
Business Address |
City, State, Zip |
|
T24m |
| Fact Name | Details |
|---|---|
| Purpose | This form collects employment information to assess eligibility for Florida KidCare health insurance. |
| Submission | Submit the completed form to Florida KidCare at P O Box 591, Tallahassee, Florida, 32302-0591. |
| Section A | Section A must be filled out by the employee, including their family account number and signature. |
| Employer's Role | Employers must complete Section B, providing necessary employment details about the employee. |
| Payment Frequency | Employers must indicate how often the employee is paid: daily, weekly, bi-weekly, monthly, or other. |
| Gross Pay Rate | Employers need to state the employee's gross pay rate and the corresponding time frame (hour, day, week, etc.). |
| Accuracy Statement | Employers must confirm the accuracy of the information provided and acknowledge the consequences of false information. |
| Required Signatures | Both the employer and employee must sign the form to validate the information and consent. |
| Legal Reference | This form is governed by Florida Statutes Chapter 409, which pertains to public assistance programs. |
| Exemption | If recent pay stubs are provided, the employment statement form is not required. |
Wage Assignment Laws by State - This form serves as a petition for relief from court-ordered automatic salary deductions in Florida.
Radon Gas Disclosure Florida - Nonresidential facilities have a responsibility to accurately report the age and construction details of the building concerned.