Cpe Reporting Florida Form in PDF
Cpe Reporting Florida Form in PDF
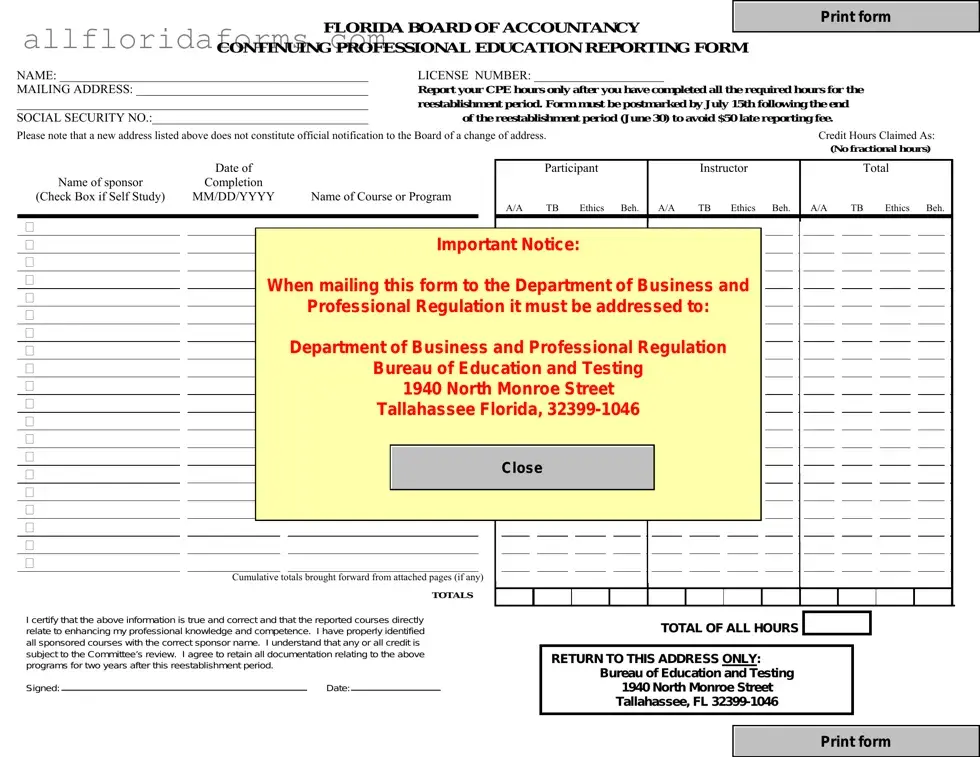
The CPE Reporting Florida form is a crucial document for licensed accountants in Florida, ensuring compliance with continuing professional education requirements. This form must be completed after all required CPE hours have been achieved during the reestablishment period, which ends on June 30. It must be postmarked by July 15 to avoid a late fee. The form collects essential information, including the licensee's name, license number, mailing address, and social security number. It also requires detailed reporting of CPE hours, categorized by type, such as accounting and auditing, ethics, and behavioral subjects. Each course listed must include the completion date, sponsor name, and whether it was a self-study course. The form emphasizes the importance of accuracy, requiring licensees to certify that the information provided is true and correct. Incomplete forms will be returned, so careful attention to detail is necessary. Furthermore, the form must be signed and dated, and any address changes must be reported separately to the Board. Overall, this document serves as a key tool for maintaining professional standards in the accounting field.
FLORIDA BOARD OF ACCOUNTANCY |
|
|
Print form |
|
|
|
|
|
|
CONTINUING PROFESSIONAL EDUCATION REPORTING FORM |
|
|
||
NAME: __________________________________________________ |
LICENSE NUMBER: _____________________ |
MAILING ADDRESS: ______________________________________ |
Report your CPE hours only after you have completed all the required hours for the |
_________________________________________________________ |
reestablishment period. Form must be postmarked by July 15th following the end |
SOCIAL SECURITY NO.:___________________________________ |
|
|
of the reestablishment period (June 30) to avoid $50 late reporting fee. |
|||||||||||||||||||||||||||||
Please note that a new address listed above does not constitute official notification to the Board of a change of address. |
|
|
|
|
|
|
Credit Hours Claimed As: |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(No fractional hours) |
||||||
|
|
Date of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name of sponsor |
|
|
|
|
|
|
|
|
Participant |
|
|
|
Instructor |
|
|
Total |
||||||||||||||||
Completion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
(Check Box if Self Study) |
MM/DD/YYYY |
|
Name of Course or Program |
A/A TB Ethics Beh. |
|
A/A |
|
TB Ethics Beh. |
A/A TB Ethics Beh. |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Important Notice: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
When mailing this form to the Department of Business and |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
Professional Regulation it must be addressed to: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Department of Business and Professional Regulation |
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
Bureau of Education and Testing |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
1940 North Monroe Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
Tallahassee Florida, |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Close |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cumulative totals brought forward from attached pages (if any)
|
|
|
|
TOTALS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that the above information is true and correct and that the reported courses directly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
TOTAL OF ALL HOURS |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
relate to enhancing my professional knowledge and competence. I have properly identified |
|
|
|
|
|
|
|
|
|
|
||||||||||
all sponsored courses with the correct sponsor name. I understand that any or all credit is |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
subject to the Committee’s review. I agree to retain all documentation relating to the above |
|
|
|
|
RETURN TO THIS ADDRESS ONLY: |
|
|
|
|
|
||||||||||
programs for two years after this reestablishment period. |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
Bureau of Education and Testing |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Signed: |
|
Date: |
|
|
|
|
|
|
|
1940 North Monroe Street |
|
|
||||||||
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
Tallahassee, FL |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print form
INSTRUCTIONS FOR COMPLETING THIS FORM
1.This form must be printed or typed and returned to the Bureau of Education & Testing. All information requested on the form must be completed. Courses must be listed directly on the form to make it complete. Incomplete forms cannot be evaluated and will be returned. (Licensees should retain a copy for their files). Xeroxed copies are acceptable. However, original signatures are required.
2.The minimum requirements for each two year reestablishment period are completion of at least 80 total hours, of which at least 20 hours must be in accounting and auditing (A/A) subjects, 4hours must be in ethics, and no more than 20 hours may be in behavioral subjects. The A/A category includes courses on financial reporting, financial auditing, the related pronouncements, and accounting for specialized industries. The Technical Business category includes courses on taxation, MAS, and general business subjects. The Behavioral category includes courses on oral and written communication, practice administration, management, and marketing. The Ethics category includes only providers and courses approved by the Florida Board of Accountancy. The list of approved courses is available on the board’s website http://www.myflorida.com/dbpr/cpa.
3.Please indicate
4.If the course was presented by an approved sponsor, please enter the sponsor code. If the sponsor was not approved leave this area blank. Note that sponsors do not report for you. You must report all courses which you wish to have recorded.
5.When listing the sponsor code, be certain to complete the blanks with the alpha letter in the first column followed by the numeric digits.
6.Credit can be claimed for two types of activity: (1) hours earned as a participant and (2) hours earned as an instructor or lecturer. If you are reporting hours of instruction, you may claim double credit for the first presentation of the course, single credit for the second presentation of the same course, and no credit thereafter except for new content (See Rule
7.List the hours claimed in the appropriate column. Report whole hours only, no fractions. Fractional hours must be rounded down to the nearest whole hour. Any fractional hour reported will be removed. Total all columns and indicate the total of all hours from all categories in the box at the bottom.
8.The form must be signed and dated. Be sure to indicate your employer or firm name.
9.You are required to notify the Board office in writing of address changes (Rule 61H126.005). A change of address on this reporting form will not constitute official notification and will not result in an address change.
10.If there are any questions regarding the use of this form, contact:
Bureau of Education & Testing
1940 N. Monroe Street
Tallahassee, Florida
Or by Phone: 850.487.1395
*Under the Federal Privacy Act, disclosure of Social Security numbers is voluntary unless specifically required by Federal statute. In this instance, social security numbers are mandatory pursuant to Title 42 United States Code, Sections 653 and 654; and sections 455.203(9), 409.2577, and 409.2598, Florida Statutes. Social Security numbers are used to allow efficient screening of applicants and licensees by a Title
DBPR FORM CPA41
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used by licensed accountants in Florida to report their Continuing Professional Education (CPE) hours. |
| Submission Deadline | The form must be postmarked by July 15th following the end of the reestablishment period, which concludes on June 30. |
| Late Fee | A late reporting fee of $50 is incurred if the form is submitted after the deadline. |
| Minimum Requirements | For each two-year reestablishment period, a minimum of 80 total hours is required, including at least 20 hours in accounting and auditing subjects and 4 hours in ethics. |
| Self-Study Courses | Self-study courses must be taken from sponsors approved by NASBA's Quality Assurance Service to qualify for credit. |
| Address Change Notification | Changing the address on this form does not officially notify the Board. Written notification is required for address changes. |
| Governing Laws | This form is governed by Florida Statutes, including sections 455.203(9), 409.2577, and 409.2598. |
Family Law Financial Affidavit Short Form Florida - The 12.902(b) form facilitates fair financial settlements and support arrangements by presenting a clear financial picture of both parties involved.
Rn Refresher Course Florida - This form requires detailed program information, including addresses, schedules, and director credentials, for complete transparency and compliance.
Form 6 Florida - Students are instructed to provide detailed personal information and their new program details at FIU for accurate processing.